Let experts handle it, then spot the difference! ORDER NOW

NSG5003 Week 9 Discussion
NSG5003 Week 9 Discussion
NSG5003 Week 9 Discussion
Neurological System Case Study – #1
Mrs. Smith is an 85-year female with a history of Hypertension, diabetes and osteoarthritis. Her daughter who cares for her reports that she became suddenly confused beginning last night. She knows her daughter but has been unable to remember her grandchildren’s names. She continuously asks her daughter “What are those kids doing in our house?”
Her mother was in and out of bed all night and slept very little. Her daughter does say that her mother seemed better this morning, but on the way to your office she became more confused again. Review of systems is significant for a dry cough for the past few days. She has not had a fever. Her appetite has been poor. Her exam is normal except for some fine crackles in her left lung base. Mrs. Smith’s daughter says” My dad had Alzheimer’s and now it looks like I am going to have to go through that with my mother”
1) What are the possibilities for change in Mrs. Smith’s current mental status?
2) What is your top differential diagnosis? Give 3 reasons why you chose that diagnosis.
3) How can you differentiate depression, dementia and delirium?
4) Explain to Mrs. Smith’s daughter what treatment is needed and what you think her prognosis is.
Effects of depression, dementia and delirium on activities of daily living in elderly patients after discharge
Abstract
Background
The three geriatric conditions, depression, dementia and delirium (3D’s), are common among hospitalized older patients and often lead to impairments of activities of daily living. The aim of this study is to explore the impact of depression, dementia and delirium on activities of daily living (ADLs) during and after hospitalization.
Methods
A prospective cohort study was conducted between 2012 and 2013 in a tertiary medical center in Taiwan. Patients who aged over 65 years and admitted to the geriatric ward were invited to this study. Geriatric Depression Scale Short Form, Mini-Mental State and Confusion Assessment Method were used to identify patients with depression, dementia and delirium on admission, respectively. Barthel Index (BI) was used to evaluate patients’ functional status on admission, at discharge, 30-day, 90-day and 180-day after discharge. Generalized Estimating Equation (GEE) was used to calculate the associations between 3 D’s and BI.
Results
One-hundred-and-forty-nine patients were included in this study. Twenty-seven patients (18.1%) had depression, 37 (24.8%) had dementia, and 85 (57.0%) had delirium. The study demonstrated that all the geriatric patients with functional decline presented gradual improvements of physical function up to 180 days after discharge. Whether depression exists did not substantially affect functional recovery after discharge, whilst either dementia or delirium could impede elder people functional status. The recovery of functional improvement in delirium or dementia was relatively irreversible when comparing with depression. Once delirium or dementia was diagnosed, poorer functional restore was expected. In brief, intensive work and strategies on modifying delirium or dementia should be put more effort as early as possible.
Conclusions
Old hospitalized patients with depression can recover well after adequate intervention. We emphasize that early detection of dementia and delirium is imperative in subsequent functional outcome, even if at or before admission. Comprehensive plan must be implemented timely.
Background
Functional decline, defined as deterioration in self-care skills, is a common and devastating problem for hospitalized elderly patients [1, 2]. It is associated with prolonged hospital stay, increased mortality, higher rates of institutionalization, and greater health care expenditure. Recent studies suggested that 34 to 50% of elderly patients experienced functional decline during hospitalization [3, 4]. The reasons for decline are often irrelevant to the patients’ admission diagnoses, but related to the underlying primary illness or iatrogenic complications during hospitalization [5, 6].
Geriatric syndromes are prevalent among older people and have been known to be associated with poor outcomes, such as readmission, increased length of stay, functional decline, hospitalization and mortality [7,8,9,10]. The most common geriatric syndromes include malnutrition, incontinence and geriatric psychiatric problems, in particular, depression, dementia and delirium [11]. The geriatric psychiatry–delirium, dementia, and depression, recognized as geriatric three D’s, frequently coexist and overlap by symptoms and caused clinical diagnosis challenging. Dementia is irreversible, and can only be prescribed by certain medication which is not beneficial in treatment outcome literally. The strategy for handling dementia should take environmental factors into consideration. Other than dementia, delirium and depression could be treated and reversible. Nevertheless, the presentation of hypoactive delirium or major depressive disorder were vague and can be easily confused by dementia. Three D’s symptoms often coexist. Once each of symptoms occurred in one old person simultaneously, the delay of diagnosis with proper intervention confer risk of functional recovery, which will lead to poor management of adverse outcomes. Hence geriatric psychiatric problems remain the most differential diagnoses in the older populations [12].
Understanding older patients who are at risk of functional decline during hospitalization is necessary before preventive strategies can be developed. Older age, lower Mini–Mental State Examination (MMSE) score, and poor nutrition status predict functional decline and deterioration of functional capacity restoration [2]. Geriatric conditions impede elder function after discharge had been well documented, several studies proposed certain useful predictors and provide unique tool in these field [8, 13,14,15]. Geriatric psychiatry had profound deterioration in functional outcome even several months after discharge, especially when co-occurrence of three D’s. Based on the past literature, we aim to discover whether functional restoration been affected by geriatric three D’s after hospitalization up to 180 days. In this study, we explore the impact of depression, dementia and delirium on functional trajectory in the hospitalized elder patients. To the best of our knowledge, this is the first study to elucidate the role of geriatric psychiatric three D’s on functional capacity 6 months after discharge. SU NSG5003 Week 9 Discussion latest
Materials and methods
Study design and population
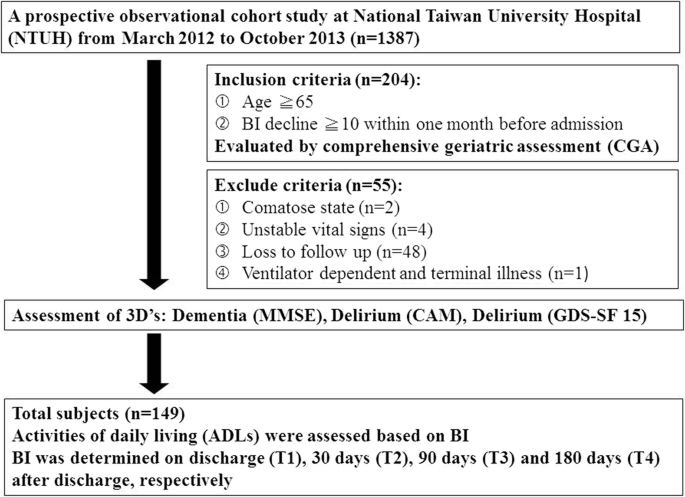
A prospective observational cohort study was conducted at National Taiwan University Hospital (NTUH) from March 2012 to October 2013. A total of 149 hospitalized patients were invited to this study. All the participants were evaluated using comprehensive geriatric assessment (CGA) [16, 17] by the geriatric interdisciplinary team. Inclusion criteria were hospitalized patients aged 65 years or older, having a Barthel Index (BI) decline more than ten points within one month before the index hospitalization (the measurement of BI decline was recorded by questionnaire when admission). Exclusion criteria were patients who were in comatose state, unstable vital signs, ventilator dependent and terminal illness (e.g. multiple organ failure, cancer with or without metastatic lesion) (Fig. 1). The patients or their proxies were informed about the details of the present study and the potential risks during the process by the clinicians, and they were provided with the written informed consents. The proxies referred to the adult children, close relatives and friends of the patients. All the participants enrolled in the study signed the informed consent form by himself/ herself or their proxies. The research ethic committee at NTUH approved the study (No. 201108057RC).
Data collection
Assessment of 3Ds
Depression was assessed according to Geriatric Depression Scale Short Form 15 (GDS-SF 15). Patients who scores more than 5 points are considered depressed [18]. Dementia or cognitive impairment was assessed according to Mini–Mental State Examination (MMSE), is a 30 points questionnaire to evaluate cognitive function with education adjusted cut-off points. Any score of 24 or more indicates normal cognition. Scores ≤9 points indicate severe, 10 to18 points was moderate, and 19 to 23 points was mild cognitive impairment [19]. Delirium was evaluated according to Confusion Assessment Method (CAM). The CAM diagnosis is based on four features: 1) acute onset and fluctuating course, 2) inattention, 3) disorganized thinking, and 4) altered level of consciousness. A diagnosis of delirium according to the CAM requires the presence of features 1, 2, and either 3 or 4 [20]..
Assessment of comorbidity and other geriatric problems
Patients who reported having comorbid illnesses such as hypertension, diabetes mellitus, stroke, coronary artery disease, chronic obstructive pulmonary disease, heart failure, atrial fibrillation, hip fracture, and Parkinson’s disease were recorded. Charlson Comorbidity Index (CCI) was also used to measure burden of disease [21].
Among other common geriatric problems, number of fall within one year prior to index admission was recorded. Hearing impairment is defined as having communication difficulties because of poor hearing with or without hearing aids. The visual impairment is conceptualized as poor eyesight despite using corrective lens.
Assessment of functional status
Activities of daily living (ADLs) (i.e. eating, transferring from bed to wheelchair, toileting, bathing, dressing, ambulation, and urination and defecation control) were assessed based on BI, and the total score of BI is 100 [22]. Ascertainment of functional decline is defined as BI decreases more than ten points in one month before admission. BI was also determined on discharge (T1), 30-day (T2), 90-day (T3) and 180-day (T4) after discharge (Fig. 1). NSG5003 Week 9 Discussion
Statistical analysis
Data were reported as number (percentage) for categorical variable and mean (standard deviation) for continuous variables. Group difference was assessed using chi-square or t-test when appropriate. The relationship between the development of ADL independence over time and the type of 3Ds was analyzed using generalized estimating equation (GEE). SU NSG5003 Week 9 Discussion latest
The interaction terms of each geriatric condition by time points (using discharge as reference category) were added to the GEE model adjusted with age and gender. The changes in functional status are significantly different for a given subgroup (of a certain geriatric condition) when a significant interaction term appears.
Finally, to investigate the associated factors with functional status over time, GEE was adopted again in which all the patients’ characteristics were adjusted including depression, dementia and delirium into one model. All the statistical analyses were conducted using SPSS software version 15 (SPSS Inc., Chicago, Illinois). Statistical significance was defined as p < 0.05.
Results
Subjects
Table 1 depicts the clinical characteristics of all participants. The mean age was 87.6 years. Among the participants, 80.5% were 81 years or older, 54.4% were female, 60.4% received less than 9 years of education, 46.3% were still married, 10.7% living alone, and 69.8% having their sons or daughters as their primary contact person. The most common comorbidities were hypertension (78.5%), stroke (60.8%), diabetes mellitus (39.9%), coronary artery disease (26.4%), and chronic obstructive pulmonary disease (15.5%). On average, each subject had 4 comorbidities and the CCI revealed a score of 4.1. NSG5003 Week 9 Discussion
More than half of the subjects (54.7%) experienced fall in the past years, and 11.5 and 29.1% of the participants had hearing and visual impairments, respectively. On average, each participant took 8.5 prescription drugs per day and the length of hospitalization was 13.8 days (Table 1).
Comparison of functional status among the 3D’s patients
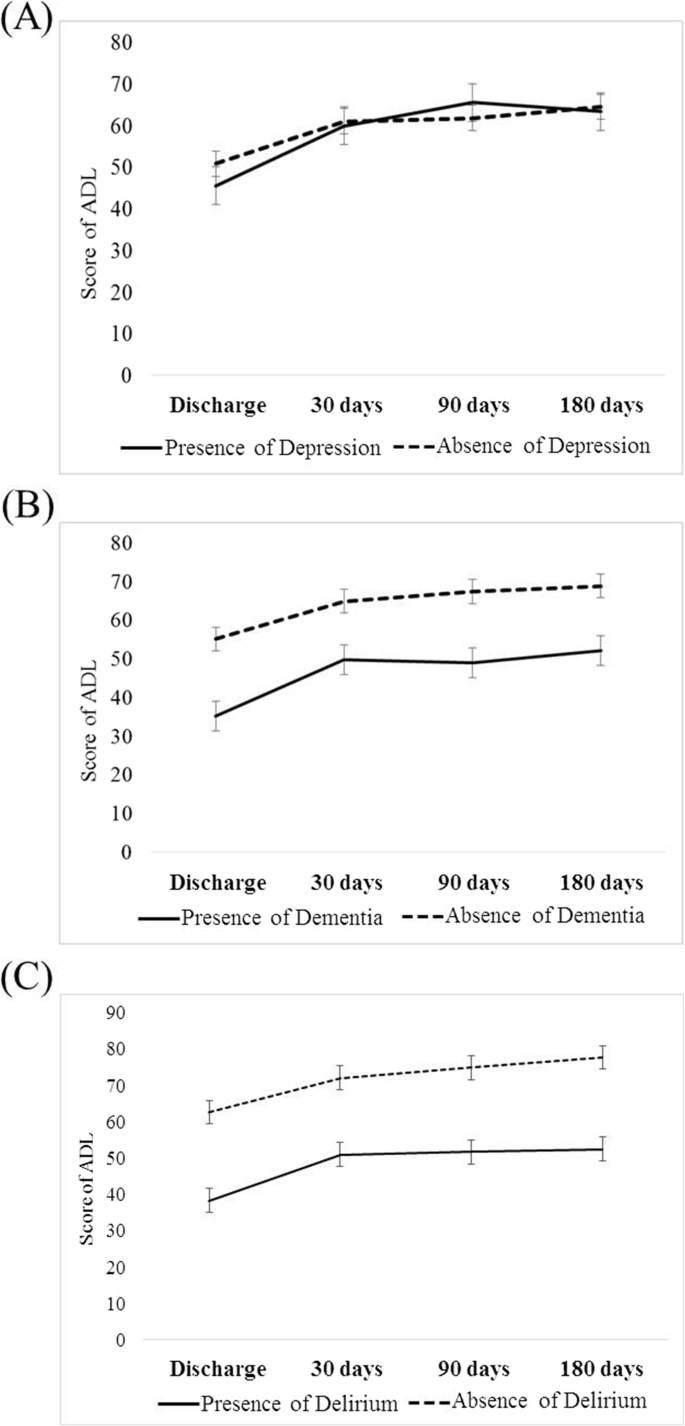
Of the 149 participants, 27 (18.1%) had depression, 37 (24.8%) had dementia, and 85 (57.0%) had delirium. The BI scores were similar among patients with or without depression in each time point even to the end of study time at 180 days. In contrast, patients with dementia or delirium demonstrated lower BI scores than those without and that the parallel gap persisted constantly up to six months after discharge (p < 0.01) (Table 2). This demonstrated a decreasing trend in functional regain after discharge (Table 2, Fig. 2 a-c). GEE was used to estimate the change in BI scores at various time points. Regardless of the presence of three D’s, the magnitude of functional improvement was not obvious in each time points in the three groups (Table 3, Fig. 2 a-c), When taking age, gender, dementia, delirium and depression into account in each model of three D’s, depression is independent from all the variables. Of note, in model of dementia group, delirium showed statistically significant (p = 0.003), and vice versa in model of delirium group (p = 0.004) (Table 3). In general, patients with delirium or dementia had worse functional status compared with those without, even though slightly improvement after discharge. On contrary, functional status remained similar to six months after discharge irrespective of depressive status. NSG5003 Week 9 Discussion
Discussion
The present study demonstrated that all the geriatric patients with functional decline presented gradual improvements of physical function up to 180 days after discharge. Whether depression exists did not substantially affect functional recovery after discharge, whilst either dementia or delirium could impede elder people functional status.SU NSG5003 Week 9 Discussion latest
The term “geriatric syndromes” contains the features of various conditions in the elder people. The causes of geriatric syndromes is multifactorial, patient-specific and situation-specific, and often lead to subsequent sequela, morbidity and poor outcomes in hospitalized elderly [10, 23]. Geriatric psychiatric problems—delirium, dementia, and depression denote the most common presentation and obscure diagnoses for older adults [12]. These syndromes may overlap and exist simultaneously or emerge exclusively in one patient, and affect or confer to the other mutually, which eventually lead to functional decline, institutionalization and even death [12, 24].
Old people suffering from one of the geriatric psychiatric problems often have poor ADL outcomes and increasing risks of death. Several studies have developed strategies to predict the outcomes of functional decline or mortality in the elderly [13, 14]. Barnes et al proposed a new strategy for prognosis, which can predict the risk of outcomes including functional recovery, dependence and death [15]. McCusker et al investigated the co-occurrence of the delirium, depression and dementia, and found that those without co-occurrence had better outcome [25]. In our study, we stratified functional decline of the hospitalized elder patients on admission and assessed the association between geriatric psychiatric problems and functional change after discharge. The patients with delirium were too confused to maintain self-care, thus a low BI score were expected. Dementia is a strong risk factor for delirium, and once delirium develops, it can accelerate and worsen physical functions [26, 27]. Similar to other studies, our finding also showed that the presence of delirium and dementia was associated with poorer functional recovery after hospitalization [28,29,30]. Slightly parallel improvements in functional trajectories after discharge among those with or without delirium or dementia were seen (Fig. 2 a-c). Once dementia and delirium present before admission, each of them impedes elder people function persistently.
To overcome these functional gaps, patients may need to consider other interventions such as rehabilitations, or as in this study, CGA. CGA is a useful tool that involves interdisciplinary diagnostic process to identify functional, medical, mental, and socio-environmental complex problems of frail elderly in order to coordinate a proper program to treat and manage for optimal outcome [16, 17, 23]. CGA is specialized in geriatric wards than general ward with geriatric teams [16]. Furthermore, direct communication, highly trained staff and effective interdisciplinary team will implicate the treatment outcome in subspecialized geriatric ward and inpatient stroke care unit [31]. CGA during hospitalization has effect on decreasing mortality, improvement function, and decreasing placement in nursing homes. The prolong effect after acute illness also reveal good impact, especially in at-risk elderly in the community [32]. Our results disclose that patients’ functional status improved regardless of their geriatric psychiatric problems, suggesting the effectiveness of CGA. SU NSG5003 Week 9 Discussion latest
On the other hand, all depressed patients improved functional outcome and as equivalent to those without depression up to 6 months after discharge, suggesting depression is a reversible disease and early intervention is crucial in reversing the functional outcome. Previous researches have highlighted the under diagnosis of depression among the elderly [33]. Although diagnosis is challenging, it is nevertheless potentially treatable morbidity in older people [34,35,36], clinical practitioner should put efforts on access to appropriate treatment. In our study, the magnitude of ADL improvement is equal in depression group after 180 days discharge. The explanations are first, the awareness of depression by caregiver that helps in coping with depression either in daily activity or taking antidepressant agents. Second, delirium and dementia have greater impact impeding functional status, whilst depression mainly influences mental function but not physical function.
Functional outcome in elder people are thought to be affected especially with more comorbidities, older age or more geriatric syndromes. Whether patients recover or maintain ADLs at an optimal state depends largely on careful assessments and plans. It is imperative that elderly patients with geriatric psychiatric condition, especially delirium and dementia should undergo rehabilitation in order to improve physical functioning. We highlighted CGA during admission in elder people, and the application was suggested effective and crucial during the whole course after discharge. The recovery of functional improvement in delirium or dementia was relatively irreversible when comparing with depression. Given the diagnosis of delirium or dementia was established, poorer functional restore was utterly expected. Hence, intensive work and strategies on modifying delirium or dementia should be put more effort as early as possible, not only by medical stuff but primary caregiver. Readily intervention with accuracy diagnosis of dementia and delirium is important. We suggest further research focusing on which intervening on depression in post-hospitalization care regain promising better functional outcomes. And, if so, whether pharmacologic or non-pharmacologic plan could lead to functional recovery should be investigated.SU NSG5003 Week 9 Discussion latest
This study has several limitations. First, the sample size was relatively small, thus the confounding variables could not draw a distinct effect on each of the 3D’s in terms of functional outcomes. Second, the patients were not evaluated by the same staff every time during CGA, thus differences in reporting data and inconsistency may occur. Reassessed using rigorous research methods with well-trained same staff can provide much more promising results. Third, the definition of each of the 3D’s might also be underestimated of the true prevalence in this study. Forth, the population had a substantial loss of follow-up for certain reasons such as rehospitalization may diminish the statistic power in this study.
Conclusion
In conclusion, old hospitalized patients with depression can recover well after adequate intervention. We emphasize that early detection of dementia and delirium is imperative in subsequent functional outcome, even if at or before admission. Comprehensive plan must be implemented timely.SU NSG5003 Week 9 Discussion latest
ADDITIONAL INSTRUCTIONS FOR THE CLASS –
Who we are
Do you handle any type of coursework?
Yes. We have posted our previous orders to display our experience. Since we have done this question before, we can also do it for you. To make sure we do it perfectly, please fill out our Order Form. Filling the order form correctly will assist our team in referencing, specifications, and future communication.Is it hard to Place an Order?
- 1. Click on “Order Now” on the main Menu and a new page will appear with an order form to be filled.
- 2. Fill in your paper’s requirements in the “PAPER INFORMATION” section and the system will calculate your order price/cost.
- 3. Fill in your paper’s academic level, deadline, and the required number of pages from the drop-down menus.
- 4. Click “FINAL STEP” to enter your registration details and get an account with us for record-keeping and then, click on “PROCEED TO CHECKOUT” at the bottom of the page.
- 5. From there, the payment sections will show, follow the guided payment process and your order will be available for our writing team to work on it.
SCORE A+ WITH HELP FROM OUR PROFESSIONAL WRITERS – NSG5003 Week 9 Discussion
We will process your orders through multiple stages and checks to ensure that what we are delivering to you, in the end, is something that is precise as you envisioned it. All of our essay writing service products are 100% original, ensuring that there is no plagiarism in them. The sources are well-researched and cited so it is interesting. Our goal is to help as many students as possible with their assignments, i.e. our prices are affordable and services premium.
- Discussion Questions (DQ)
Initial responses to the DQ should address all components of the questions asked, including a minimum of one scholarly source, and be at least 250 words. Successful responses are substantive (i.e., add something new to the discussion, engage others in the discussion, well-developed idea) and include at least one scholarly source. One or two-sentence responses, simple statements of agreement or “good post,” and responses that are off-topic will not count as substantive. Substantive responses should be at least 150 words. I encourage you to incorporate the readings from the week (as applicable) into your responses.
- Weekly Participation
Your initial responses to the mandatory DQ do not count toward participation and are graded separately. In addition to the DQ responses, you must post at least one reply to peers (or me) on three separate days, for a total of three replies. Participation posts do not require a scholarly source/citation (unless you cite someone else’s work). Part of your weekly participation includes viewing the weekly announcement and attesting to watching it in the comments. These announcements are made to ensure you understand everything that is due during the week. NSG5003 Week 9 Discussion
- APA Format and Writing Quality
Familiarize yourself with the APA format and practice using it correctly. It is used for most writing assignments for your degree. Visit the Writing Center in the Student Success Center, under the Resources tab in Loud-cloud for APA paper templates, citation examples, tips, etc. Points will be deducted for poor use of APA format or absence of APA format (if required). Cite all sources of information! When in doubt, cite the source. Paraphrasing also requires a citation. I highly recommend using the APA Publication Manual, 6th edition.
- Use of Direct Quotes
I discourage over-utilization of direct quotes in DQs and assignments at the Master’s level and deduct points accordingly. As Masters’ level students, it is important that you be able to critically analyze and interpret information from journal articles and other resources. Simply restating someone else’s words does not demonstrate an understanding of the content or critical analysis of the content. It is best to paraphrase content and cite your source. NSG5003 Week 9 Discussion
- LopesWrite Policy
For assignments that need to be submitted to Lopes Write, please be sure you have received your report and Similarity Index (SI) percentage BEFORE you do a “final submit” to me. Once you have received your report, please review it. This report will show you grammatical, punctuation, and spelling errors that can easily be fixed. Take the extra few minutes to review instead of getting counted off for these mistakes. Review your similarities. Did you forget to cite something? Did you not paraphrase well enough? Is your paper made up of someone else’s thoughts more than your own? Visit the Writing Center in the Student Success Center, under the Resources tab in Loud-cloud for tips on improving your paper and SI score. NSG5003 Week 9 Discussion
- Late Policy
The university’s policy on late assignments is a 10% penalty PER DAY LATE. This also applies to late DQ replies. Please communicate with me if you anticipate having to submit an assignment late. I am happy to be flexible, with advance notice. We may be able to work out an extension based on extenuating circumstances. If you do not communicate with me before submitting an assignment late, the GCU late policy will be in effect. I do not accept assignments that are two or more weeks late unless we have worked out an extension. As per policy, no assignments are accepted after the last day of class. Any assignment submitted after midnight on the last day of class will not be accepted for grading.
- Communication
Communication is so very important. There are multiple ways to communicate with me: Questions to Instructor Forum: This is a great place to ask course content or assignment questions. If you have a question, there is a good chance one of your peers does as well. This is a public forum for the class. Individual Forum: This is a private forum to ask me questions or send me messages. This will be checked at least once every 24 hours. NSG5003 Week 9 Discussion
- Guarantee


- Zero Plagiarism
- On-time delivery
- A-Grade Papers
- Free Revision
- 24/7 Support
- 100% Confidentiality
- Professional Writers
- Services Offered
- Custom paper writing
- Question and answers
- Essay paper writing
- Editing and proofreading
- Plagiarism removal services
- Multiple answer questions
We will process your orders through multiple stages and checks to ensure that what we are delivering to you, in the end, is something that is precise as you envisioned it. All of our essay writing service products are 100% original, ensuring that there is no plagiarism in them. The sources are well-researched and cited so it is interesting. Our goal is to help as many students as possible with their assignments, i.e. our prices are affordable and services premium. NSG5003 Week 9 Discussion
Looking for a Similar Assignment? Order a custom-written, plagiarism-free paper